May 27, 2016 | Summer 2016
Our first study in Sierra Leone involved identifying the current pathways individuals take to screen for, diagnose and treat diabetes in Sierra Leone.
This study answered the following question: What is the current system (or baseline) used to screen for, diagnose and treat individuals with diabetes in Sierra Leone?
Interviews were conducted with community health workers (CHWs), community members, pharmacists, doctors and nurses at hospitals and PHUs. The interview questions focused on isolating and tracking the step-by-step process that is used to 1) diagnose individuals with diabetes and 2) treat individuals with diabetes.
Semi-structured interviews were conducted during the first ten days of field work with CHWs, community members, doctors and nurses at local clinics, diabetes support groups, pharmacists, and other entities in the health network. To identify interview participants, we partnered with the District Medical Officer and World Hope International and were connected to doctors, nurses, and pharmacists in the health network.
Through these interviews, we gathered insights not only on the screening pathways for diabetes, but also on the passion of community members, doctors, nurses, and CHOs to enact widespread screening and treatment of diabetes. We talked to a community member who started a Diabetes Association, which is a forum where patients with diabetes talk about their challenges, learn ways to improve their health, and donate money for those who are unable to pay for medication or families of those who have died from diabetes. We got tremendous insight from CHOs as they explained the fatalities that occurred as a result of diabetes and the barriers individuals face to receive health care. We spoke with doctors and nurses who are working hard to provide treatment options, even if it means travelling to Freetown to get medication or donating their time to give free screening. It was evident that individuals of the health care system and community members have deep care and concern about diabetes and are ready to take action against it. They are excited about the research we are doing in order to look at possible ways to implement available screening.
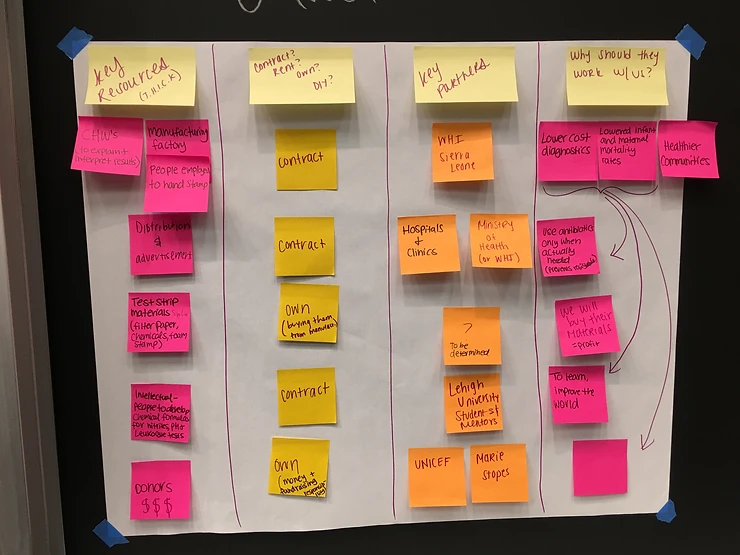
Our second study focused on determining the system response to off-the-shelf diabetes screening strips and assessing the changes in health-seeking behavior of individuals who are screened for diabetes. This study has been initiated by the whole team members and will be fully carried out by Eric through early August. So far we have had initial meetings at all 8 PHUs, gotten all training and screening materials together, and planned further actions for the rest of the summer. Eric will be initiating meetings with the pharmacies in Makeni. The full study is outlined below:
The results from Study 1 were applied to Study 2, where we looked for community responses to the integration of diabetes screening strips through different locations of the health care system and at different costs. There was a free and paid (Le 2000) option for each scenario. To study the rural community, we met with the CHO and the staff in charge at each PHU and explained the scenario that was to take place at their PHU. Next, we went through a training where the PHU staff was trained to use the diabetes screening strips, blood glucose strips, and through the desired process for each screening. Based on the results of this study, we hope to determine the viability of a social enterprise that works to establish nationwide diabetes screening, diagnosis, and treatment plans in Sierra Leone via the sale of urinalysis test strips.
The screening process includes getting a urine sample, dipping the urinalysis strip in the sample, and interpreting the color change on the strip. If the testing is positive, as indicated by a user’s guide that is provided to them, the individual will have the opportunity to take a blood glucose test. The PHU worker will document the results of the tests as well as other provided questions in a notebook that will be collected at the end of the screening period.
Scenario 1: Poster The first of these scenarios was a passive approach, in which only a poster was put up at the chosen PHU. In this scenario it was made clear that there should not be any communication through CHW and town criers to the community. The intention of this scenarios was to see a poster’s ability to communicate a message to the community.
Scenario 2: PHU Outreach The next scenario was PHU outreach, in which the PHU goes for its regular outreach but also holds diabetes screening on site. For this scenario it was communicated that there should not be any spread of word of the diabetes screening by the CHWs or town criers. For this scenario, PHUs with no or a limited number of CHWs were chosen.
Scenario 3: CHW Outreach In another option, the diabetes screening occurred at the PHU and was communication through CHWs. CHWs will be told to tell the members of their community that diabetes screening would be held at the PHU. Individuals who were interested in getting screened at the PHU would travel there to be screened.
Scenario 4: PHU and CHW Outreach The final scenario combines PHU outreach with CHWs communicating the information with the individuals of the community. CHWs will make their normal announcement that there will be a PHU outreach and say that there is diabetes screening available at this outreach. Individuals can be screened on the day of the outreach.
Scenario 5: Pharmacy There were two urban scenarios, in which pharmacies supplied the diabetes screening strips and completed the screening at their pharmacy. If there is a positive screening, the individual would be referred to the local hospital. At one of the pharmacies there is a set price of 2000 Leones and the other pharmacy has the freedom to set their own price for the screening based on their knowledge of the market. They will go through the same screening process, except they will refer individual to the local hospital to have the blood test to verify the strips results. Through these results we hope to be able to develop a sustainable model so that this screening can be available to every community member.
Our test strips team took a snap with the wonderful PHU workers after our first training.