
Today we travelled three and a half hours to Freetown to visit the Aberdeen Women’s Center (AWC), meet with the Sierra Leone Sickle Cell Society (SLSCS), and speak with the manager from Enable the Children.
AWC is a NGO-funded, maternity and children’s hospital which provides free care to women and children from the slums of Freetown. While we were there, we spoke with Dr. Sandra Lako, a physician in the pediatric ward, Musa, a lab technician, and Margaret, a nurse in the maternity ward.
 Dr. Lako has been working in Sierra Leone since 2005, and is currently writing her dissertation on sickle cell anemia in Sierra Leone. She told us that sickle cell goes unrecognized from a government perspective in Sierra Leone, but the AWC hospital has there own small sickle cell program. For this program, if a child is suspected to have sickle cell (due to bone pain, family history, or severe anemia), they will perform the sickling test. Dr. Lako told us that at her hospital, the children are typically suspected to have sickle cell and are sent for testing between the ages of 2 and 5.
Dr. Lako has been working in Sierra Leone since 2005, and is currently writing her dissertation on sickle cell anemia in Sierra Leone. She told us that sickle cell goes unrecognized from a government perspective in Sierra Leone, but the AWC hospital has there own small sickle cell program. For this program, if a child is suspected to have sickle cell (due to bone pain, family history, or severe anemia), they will perform the sickling test. Dr. Lako told us that at her hospital, the children are typically suspected to have sickle cell and are sent for testing between the ages of 2 and 5.
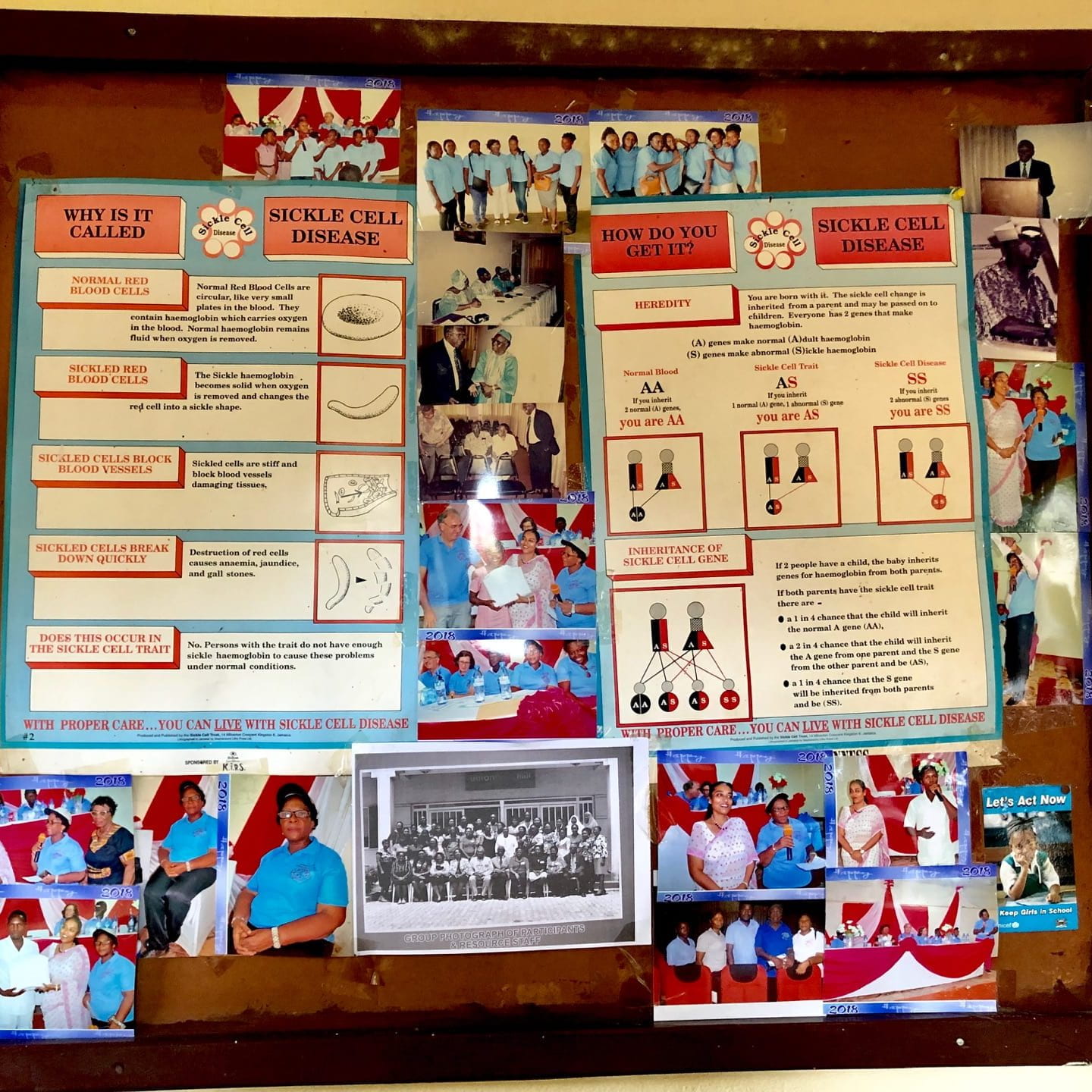
Musa, the lab technician, was able to show us this sickling test in the lab. For this test, the lab technician has to mix a blood sample with sodium metabisulphite. Sodium metabisulphite induces red blood cells containing HbS (sickle cell hemoglobin) to take on their sickle-shape. After 45 minutes, the lab technician looks at the sample under a microscope and checks to see if any of the red blood cells are sickle-shaped.
In addition to being time-intensive, this test also cannot distinguish between individuals with sickle cell disease (SS or SC) and sickle cell trait (AS). Therefore if a patient receives a positive result, they are sent to the Sickle Cell Society were they will send the patient to a local lab for Hb electrophoresis (the gold-standard test for diagnosing sickle cell) for free or an amount they are able to pay. After receiving their results they return to the Sickle Cell Society for genetic counseling and then AWC to be put on a treatment plan. Then, if one of these patients diagnosed with sickle cell comes into AWC, they are prioritized, and typically receive IV fluids and pain relief for crises.
 Margaret, a nurse in the maternity ward, also told us about the screening program they have for pregnant women. At AWC, all women who come in for antenatal care are sent for three tests: Hb levels, malaria, and sickling. If the sickling test comes back positive, they make sure not to give the woman iron during pregnancy, and to give her folic acid instead.
Margaret, a nurse in the maternity ward, also told us about the screening program they have for pregnant women. At AWC, all women who come in for antenatal care are sent for three tests: Hb levels, malaria, and sickling. If the sickling test comes back positive, they make sure not to give the woman iron during pregnancy, and to give her folic acid instead.
When we asked if they follow up with newborn screening for the babies of sickle cell mothers, Dr. Lako and Margaret said that they didn’t, but that they should sit down soon in order to close that gap in their care.
Another interesting thing which Margaret mentioned was about home births. AWC is the only specialized fistula repair center in the entire country, and therefore they get patients from all over the country. Margaret told us that a lot of these cases come from rural villages, where a high percentage of women give birth at home. Although she said that the number of individuals giving birth at home has decreased, it is important for us to know that many women still give birth at home, since we want the device to be a newborn screening tool.
After this visit, we were lucky enough to visit the Sickle Cell Society (SLSCS) and learn a little more about what happens when patients are referred there. At the SLSCS, we met with a team of nurses and Sister Amelia Gabba, the coordinator for the sickle cell program in Freetown.
When we arrived, Amelia showed us around the clinic and explained how they help their patients. She told us that all patients who don’t have a confirmed diagnosis are first referred to a local lab where they can be diagnosed for 250,000 Leones (around $25). The patient usually pays for this test themselves, but if they can’t, the clinic will cover it. Additionally, Amelia estimated that the highest price an affordable test should be was 50,000 Leones (around $5).

Once an individual has received a positive diagnosis via electrophoresis, they are taken to the genetic counseling room, where they teach individuals about how sickle cell is passed on from both parents. According to Amelia, in Sierra Leone the men will often blame the women if there is something wrong with the child, and will sometimes leave the family claiming that the woman has been unfaithful. However, by explaining the genetic cause of sickle cell (you must inherit the sickle cell gene from both the mother and father), they hope to stop some of these negative misconceptions.
In addition to genetic counseling (the SLSCS has the only two genetic counselors in the country), they also teach the families about hygiene and using bed nets (in order to reduce the risk for infection). After the initial consultation, the patient then comes in to the center every month for a check up and to receive treatment (penicillin prophylaxis, folic acid, and malaria prophylaxis). We also asked why they didn’t use hydroxyurea to treat their patients (a drug which increases fetal hemoglobin levels and therefore reduces the amount of pain crisis), and Amelia told us that it was too expensive and involved too much follow up and training (including doing cell counts frequently).

With these treatments, Amelia told us that she estimated the life expectancy of her patients was around 50. One problem which she did notice, however, was that a lot of individuals did not stick to their treatments. This was especially problematic with patients in their 20s and 30s, who may stop treatment because their symptoms have improved so much.
Amelia also made some very interesting comments when we asked her about the importance of a newborn screening program for sickle cell. First, she said that knowing whether a person had the trait was very important, as it would allow people to realize how big of an issue it is. Additionally, since women are often blamed if a child is unhealthy, a universal program where men and women are both identified as sickle cell carriers would be especially important at breaking stereotypes. Another point she stressed was that a newborn screening device would not be successful without follow up care and established facilities to handle sickle cell patients.
 Finally, we met with Anna Vines from Enable the Children. Enable the Children provides home-based therapy to kids with disabilities. In Sierra Leone, children with disabilities are highly stigmatized, seen as not worth investing in, and sometimes “seen as devils”. This meeting was applicable to our project since people with sickle cell are also often stigmatized and seen as demonic. Additionally, Enable the Children does occasionally work with sickle cell patients who have brain injuries as a result of strokes (a common side effect of sickle cell).
Finally, we met with Anna Vines from Enable the Children. Enable the Children provides home-based therapy to kids with disabilities. In Sierra Leone, children with disabilities are highly stigmatized, seen as not worth investing in, and sometimes “seen as devils”. This meeting was applicable to our project since people with sickle cell are also often stigmatized and seen as demonic. Additionally, Enable the Children does occasionally work with sickle cell patients who have brain injuries as a result of strokes (a common side effect of sickle cell).
Anna Vines also gave us a lot of information on sickle cell, traditional healers, and the healthcare system, as well as some advice. She told us that many people deny that they have sickle cell because they are seen as a weaker group. She also told us that traditional healers are often people’s first point of call, and that many of them truly believe that kids with sickle cell and other disabilities are demonic. They have a special ceremony for kids with disabilities, where they return the child to the devil (basically kill them). Additionally, she told us about challenges we may encounter with the healthcare system. Specifically, she told us that there are a lot of nurses who really don’t care about their jobs, and some of them will tell parents that their child is a demon if they have a disability.



Although most of these comments probably only reflect a small subset of the population, and may not be as applicable to sickle cell patients, she did give us some advice on how to handle these stigmas and other challenges in the future. In order to minimize misconceptions, Anna recommended that we include an information booklet as part of our program. Although she agreed that an individual knowing that they have sickle cell is important, she recommended that we give some thought on how to implement a diagnostic device in order to avoid people panicking about their diagnosis and doing bad things. She also warned us that people in Sierra Leone will often give up on preventative treatments, since they don’t see effects directly and don’t realize that they will help in the long run. With these comments, we will be sure to include an educational program with our diagnostic device.
Not only was today incredibly helpful towards our project goals, but it was also exciting to visit Freetown. The drive into the capital was beautiful, and the city itself was surrounded by mountains and beaches! To top it all off, after weeks of only eating rice and beans, we were finally able to go to a restaurant which was known for selling “safe” meat, and so we were all able to enjoy some chicken shawarma!